
The Four Stages of Male Sexual Response
Men and women share numerous aspects of the developmental life, and it results that their anatomical features are not so different from each other. For this reason, their sexual responses bear similarities and one may consider the existence of a basic human sexual response with male and female variations. In this webpage, we will focus on male sexual response.
Sexual response requires the human body to undergo numerous physiological changes, which form a typical pattern, which involves build-up of tension and ends in a release of this tension. It is important to bear in mind that this experience is continuous and that any divisions into stages are artificial and purely drawn for studying purposes. However, in an attempt to develop insight into the processes involved in this response, researchers chose to divide this pattern into four different phases. The following description of the male sexual response is founded on the four-phase division proposed by Masters and Johnson, although this model may later be refined with additional distinctions.
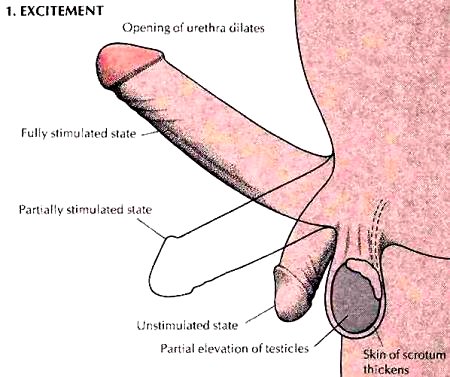
Stage 1: Excitation
Sexual excitement can build up gradually over time, but it may also increase steeply and unexpectedly, particularly in the case of younger males. An interesting fact is that some individuals deliberately distract themselves in order to prolong the process of being aroused.The excitement phase (as well as the following plateau phase) is marked by vasocongestion (swelling of the genitals with blood), myotonia (muscle tension), along with rises in heart rate, blood pressure and ventilation.This phase is also characterised by fluid secretion by the bulbourethral gland.The excitement phase may be initiated by a broad spectrum of erotic stimuli, ranging from touch, sights, sounds, aromas and even thoughts or dreams.Sexual excitement may be decreased by external interferences or sudden anxieties or apprehensions, but past its early stages, these negative influences become less effective as tension builds up and the individual becomes more uninhibited.The most obvious sign of sexual excitement is erection of the penis, which enables entry of the vagina.
 Erection represents an autonomic reflex predominantly mediated by parasympathetic fibres which run alongside the deep and helicine arteries of the penis.These fibres cause secretion of nitrous oxide (NO), leading to the relaxation of the deep arteries and lacunae.Whether this event is enough to cause erection, or whether blocking outflow of blood from the penis is also required, remains open to debate.One hypothesis supports that, as the lacunae in the proximity of the deep arteries fill with blood, they compress lacunae located closer to the periphery of the erectile tissue.From there, blood leaves the erectile tissue, therefore the compression of peripheral lacunae enhance retention of blood in the penis.Their compression is rendered more efficient due to the fact that each corpus cavernosum is wrapped in the tunica albuginea, which fits over the the erectile tissue like a tight fibrous sleeve, contributing to its tension and firmness.Additionally, the bulbospongiosus and the ischiocavernosus muscles also aid in erection by compressing the root of the penis and forcing blood forward in the shaft.
Erection represents an autonomic reflex predominantly mediated by parasympathetic fibres which run alongside the deep and helicine arteries of the penis.These fibres cause secretion of nitrous oxide (NO), leading to the relaxation of the deep arteries and lacunae.Whether this event is enough to cause erection, or whether blocking outflow of blood from the penis is also required, remains open to debate.One hypothesis supports that, as the lacunae in the proximity of the deep arteries fill with blood, they compress lacunae located closer to the periphery of the erectile tissue.From there, blood leaves the erectile tissue, therefore the compression of peripheral lacunae enhance retention of blood in the penis.Their compression is rendered more efficient due to the fact that each corpus cavernosum is wrapped in the tunica albuginea, which fits over the the erectile tissue like a tight fibrous sleeve, contributing to its tension and firmness.Additionally, the bulbospongiosus and the ischiocavernosus muscles also aid in erection by compressing the root of the penis and forcing blood forward in the shaft.
Simultaneously to the enlargement of the corpora cavernosa, the penis undergoes enlargement, becomes rigid, and elevated to an angle conducive to entry in the vagina. Once intromission is performed, the tactile and pressure sensations produced by the vaginal wall on the penis further accentuate the erection reflex. The corpus spongiosum, which possessed neither central artery nor tunica albuginea, becomes more visible as it swells. It adopts an appearance similar to a cordlike ridge along the ventral surface of the penis, although it does not become nearly as engorged and stiffened as the corpora cavernosa.Vasocongestion is not restricted to the penis, extending to the testes, which also undergo up to 50% enlargement during excitation.
As sexual excitement rises, muscular tension undergoes a corresponding increase.Pulse rate, blood pressure also increase, along with additional symptoms experienced by most men, known as ‘sex flush’.This corresponds to a red rash, flush, usually starting from the lower abdomen, spreading to the neck, face, and even shoulders, arms and thighs.The onset of the sex flush may occur in the late excitement phase but it is more often observed a bit later (in the plateau phase, delt with in the subsequent section). Note, however, that in some cases, no sex flush occurs.This observation also applies to another phenomenon: the erection of nipples, which may appear towards the end of the excitement phase or plateau phase, lasting through the following phases.
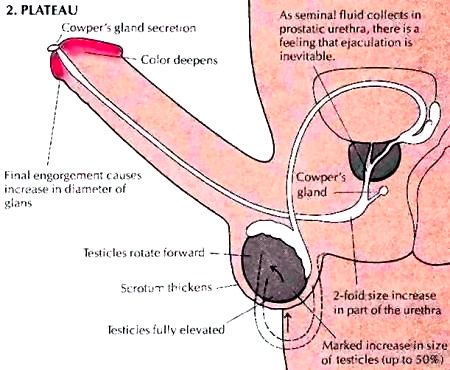
Stage 2: Plateau
The plateau phase constitutes a continuation of the excitation phase.The word plateau is used here to highlight the fact that a certain level of excitation has been achieved which is maintain for a certain time before the orgasm stage takes place.Once the stage of plateau is reached, the individual is not longer easily distracted and gradually becomes more focused to the sexual experience.With increasing stimulation, the entire body then undergoes a rise in muscular tension, both voluntary and involuntary. The pulse and blood pressure carry on rising, while respiratory rate also increases. This phase may also be marked by increased vasocongestion and myotonia.
During this phase the erect penis does not experience any additional major change, as opposed to the testicles, which swell considerably, pulled closer to the abdomen. The bulbourethral (Cowper’s) gland begins to secrete drops of a clear viscid liquid. These appear at the tip of the penis and may contain stray sperm cells. The previously mentioned sex flush may now be observable, depending upon individual variation.
Stage 3: Orgasm
The orgasm (Greek: ‘lustful excitement’) phase corresponds to the sudden release of muscular tension and nervous tension, located at the pinnacle of sexual excitement.The experience evokes the most intense physical pleasure sensation known to humans, both males and females. It may only last for a few seconds and is experienced as a short seizure or quick series of convulsions involving the whole body, succeeded by complete relaxation. The orgasm, or climax, corresponds to an intense reaction lasting about 3 to 15 seconds that is usually marked by the discharge of semen. During this phase, the heart rate may increase up to 180 beats/min, accompanying by a proportional rise in blood pressure and respiratory rate which may reach 40 breaths/min. From the stand point of offspring production, ejaculation of semen into the vagina constitutes the most significant aspect of the male sexual response. Ejaculation constitutes a two-step process comprised of an emission stage and expulsion stage.In emission, the sympathetic nervous system increases peristalsis in the smooth muscle of the ductus deferens. This phenomenon is responsible for the propulsion of sperm from the tail of the epididymus along the ductus and into the ampulla.Contractions of the ampulla in turn propel the sperm into the prostatic urethra.Then, contractions of the prostate gland force prostatic fluid into the urethra.Secretions originating from the seminal vesicles also the semen shortly after the prostatic secretion has taken place.The contractions and seminal flow in this phase create an urgent sensation which makes ejaculation inevitable.Semen in the urethra activates somatic and sympathetic reflexes which result in its expulsion.
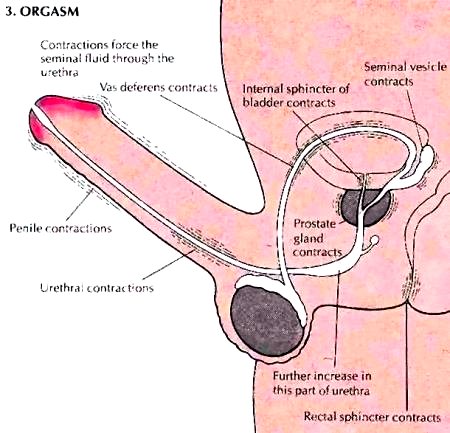
Sensory signals travelling to the spinal cord through the internal pudental nerve reach an integrating center in the upper lumbar region.Sympathetic nerve fibres carry motor signals from this point out to the prostate gland and seminal vesicles, triggering the smooth muscle in their walls to express more fluid into the urethra. The sympathetic reflex is also involved in the constriction of the internal urethral sphincter so that urine cannot enter the urethra and semen the bladder.Somatic motor signals leave the third and fourth sacral segments of the spinal cord to travel to the bulbospongiosus, ischiocavernosus and leveator ani muscles.The bulbospongiosus, which surrounds the root of the corpus spongiosum, undergoes five or six strong, spasmodic contractions that compress the urethra and forcibly expel the semen. Most sperm are in the first millimetre of semen, mixed primarily with prostatic fluid.The seminal vesicle secretion follows to flush the major part of the sperm remainder from the ejaculatory duct to the urethra.It is however important to note that some sperm may seep from the penis prior to ejaculation. Orgasm is accompanied by an intense feeling of release from tension.Although in sexually mature males, the orgasm event is associated with ejaculation (Latin: throwing out) of semen, it is important to observe that these events constitute two distinct components of the male sexual response. Although they usually occur together, it is possible to experience all the sensations of orgasm without ejaculation, and ejaculation may usually occur with little or no sensation of orgasm.
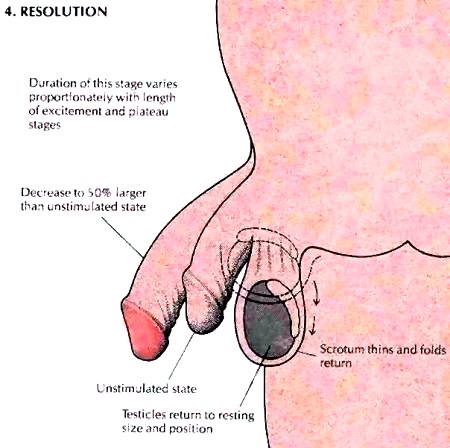
Stage 4: Resolution
Following the orgasm phase, the sexual organs as well as the rest of the body require a few minutes to return to the starting, unexcited state. The length of this ‘resolution’ phase is directly correlated to that of the excitement phase. One of the key, most noticeable features involved in this phase corresponds to the loss of erection. The latter occurs in two stages. The major loss takes place immediately after ejaculation, although the penis remains firm.This firmness may persist, particularly in cases where the initial excitement and plateau phases were prolonged, whereas other activities or distractions rapidly complete erection loss.
This phase is also marked by the fast disappearance of the sex flush, whereas eventual nipple erection persists for some time. Muscular tension in the body subsides, as breathing rate, pulse, and blood pressure drop to normal. Certain males experience sweating immediately following ejaculation, which is usually restricted to the palms and soles of the feet.
Finally, it is important to mention that, following orgasm, males undergo a ‘refractory period’. The latter, which extends largely into the resolution phase, is responsible for men’s inability to respond to any additional or new sexual stimulation, meaning no erection or no ejaculation can occur in the moments directly following the previous ejaculation. The length of the refractory period is subject to individual variation. It may be short in younger subject whereas it tends to rise in individuals of increasing age.